
Skillful Management of Chest Tubes: A Practical Nursing Guide
Nurses who work in acute care, critical care, and post-operative settings need to be able to carefully and expertly handle chest tubes. This complete guide gives a thorough look at chest tube care and is designed for nurses who want to do their jobs better in the hospital.
What chest tubes are for and when they should be used
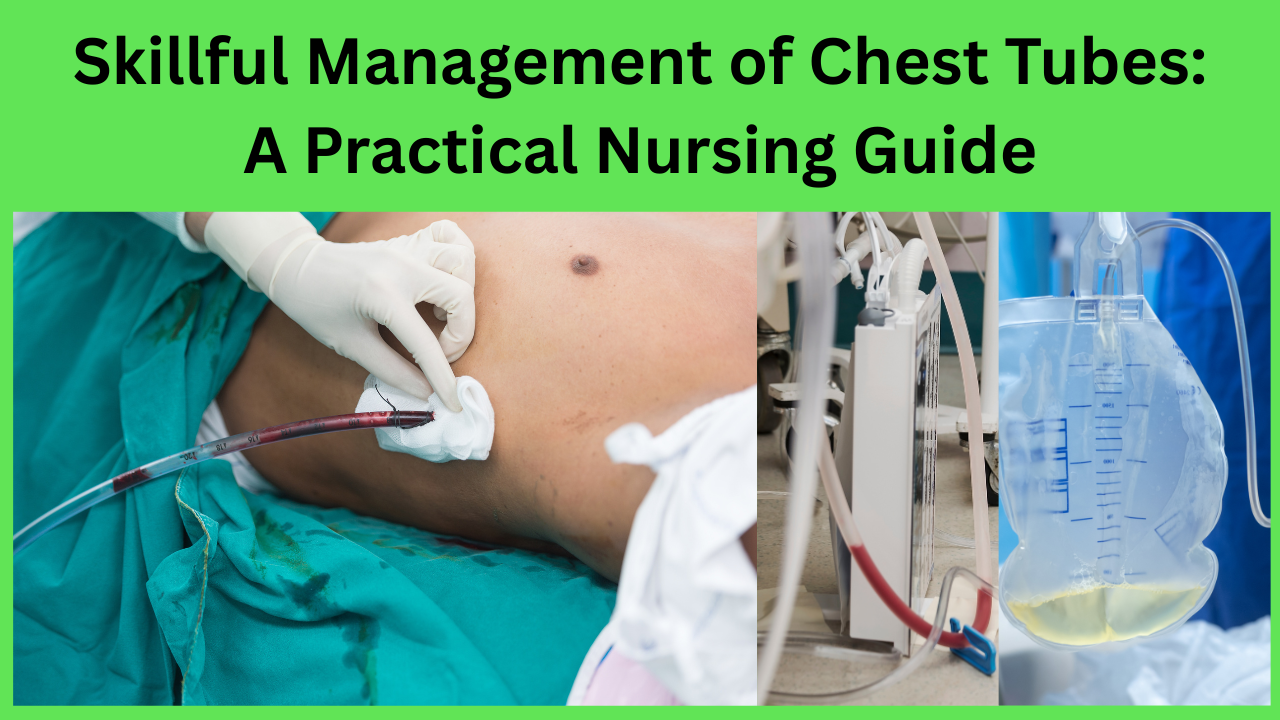
A chest tube, also known as a thoracostomy tube, is put into the pleural area to drain air, fluid, blood, or pus. The procedure helps lower the pressure inside the thorax and let the lungs expand again. Some common diseases that need a chest tube aare
The pneumothorax
Chest humps
Fluid in the pleura
Empyema
Drainage after surgery (like a thoracotomy or heart surgery)
The treatment’s success rests a lot on careful nursing care, setting up the system correctly, and constant monitoring.
Best Practices for Preparation and Setup for Inserting a Chest Tube
Before putting in a chest tube, nurses must make sure:
Consent and education: The patient receives information about what’s happening and, if necessary, permission to continue.
Positioning: Usually in a high Fowler’s or semi-Fowler’s position, with the arm raised to show the site of entry.
Please set up the chest drainage system and suction, prepare a clean tray, and have the local anesthetic, PPE, sterile gloves, and dressings ready.
Key steps for setting up:
SSafelyconnect the chest tube to the drainage system.
If necessary, prime the system (this is especially important for wet sucking systems).
Make sure that the collection room is always below the level of the chest to stop backflow.

Different kinds of chest drains
Knowing how the system works helps doctors make better decisions:
The Water Seal System lets air or fluid leave the pleural space only in one direction.
The seal chamber requires clean water.
Bubbles could mean there is an air leak.
Dry pPressureSystem: Instead of water, a mechanical regulator is used to control the pressure.
The substance is less likely to evaporate and is easy to move around.
The Heimlich Valve
A one-way valve used to treat pneumothorax in ambulatory patients.
This treatment is effective for small pneumothoraces.
Nursing Duties: Keeping an eye on things and fixing problems
Nurses are the first people who check on chest tubes. Important jobs are:
1. Evaluation of Drainage
Write down how much, what color, and how thick the drainage is.
You should consult a doctor immediately if the drainage exceeds 100 mL/hour or occurs suddenly.
Watch out for fluid that appears milky (chylothorax), pus-filled (empyema), or red (hemothorax).
2. Observation of the Water Seal Chamber
It’s normal for the water level to fluctuate (rise and fall with breathing).
Tidaling may not happen whether there is a blockage or full lung re-expansion.
Continuous popping points to an air leak.
3. Taking care of air leaks
Shortly clamp the chest tube to find the leak’s source.
Check the insert spot and connections.
Please inform the doctor if it persists.
4. Evaluation of breathing
Listen for breath sounds.
Monitor the breathing rate, effort, and oxygen level.
Be vigilant for any indications of pain, deformity, or subcutaneous emphysema.
5. Dressing and taking care of the wound
Keep the area around the injection site clean with a dressing.
As directed or when they get dirty, replace dressings.
Look for redness, warmth, or drainage as signs of an illness.
How to Fix Common Chest Tube Problems
Dislodging the Tube
Put petroleum gauze and a clean bandage over the wound.
Call the doctor or nurse right away.
Be vigilant for any indications of a stress pneumothorax.
No Drainage: Look for kinks or loops that depend on each other.
Only milk the tube if the organization says it’s okay.
Check for blockages or the growth of clots.
Everything fails.
Get back to a standing position.
Check the chambers and fluid amounts.
Notify pthe providerif it’s been hacked.
Rapid deterioration of the patient
Check for kinks, loose parts, or problems with the system.
Give the person air and raise the head of the bed.
Quickly let the medical team know.
Chest Tube Removal: Nursing Support and Post-Care Nurses assist in preparing patients for chest tube removal and monitor them throughout the process. This usually happens when:
The lungs are fully open.
Drainage is very low (less than 100 mL/day on average).
There is no air leak.
Before removal Role of Nursing
Please provide a response and manage stress effectively.
Treat pain ahead of time.
Help the patient get into the right position (semi-Fowler’s).
Make sure the right tools are available, like a suture set and an occlusive covering.
Care after removal
Put on a sealed dressing right away after taking it off.
Watch the person’s breathing and the results of the chest x-ray.
If you observe any of these indicators, you might be experiencing reaccumulation.
Teaching the patient and their family
Education is important for healing and avoiding problems:
Teach the person not to pull on or mess with the tube.
Encourage activities like coughing and deep breathing.
Show how to use a reward spirometer.
Tell them about the signs of problems, such as fever, chest pain, or more shortness of breath.
Instructions for Documentation for Chest Tube Management
Accurate and thorough documentation ensures the continuation of care.
Date and time of adding or removing
Size of the chest tube and where to put it in
What kind of water system is used
Setting for suction (if needed)
How much, what kind, and what color the drainage is
Findings from the respiratory and pain assessments
Educating the patient and their reactions to treatment
Best Ways to Avoid Getting Infections
To stop hospital-acquired illnesses (HAIs), do the following:
Clean your hands before and after using the system.
Putting on clean gloves to change a dressing.
Check the insertion spot every day.
It is important to keep systems covered to lower the risk of contamination.
It is important to know how to take care of chest tubes.
Managing a chest tube well is an important nurse skill that keeps patients safe and helps them get better in respiratory and thoracic conditions. As long as they are careful, constantly monitor the situation, and adhere to the rules, nurses can move quickly and expertly at every stage of care, from insertion to removal.
FAQ:
1. What is a chest tube used for in nurse care?
Answer: Nurses use a chest tube to remove air, blood, fluid, or pus from the pleural area. This approach helps a collapsed lung get back to normal size and breathing. It is critical for nurses to know how to handle situations like pneumothorax, hemothorax, pleural effusion, and drainage after surgery.
2. What are the most important things a nurse needs to do when managing a chest tube?
Answer: Nurses are responsible for monitoring drains, ensuring the system functions properly, searching for air leaks, monitoring the patient’s breathing, changing dressings, preventing infection, and instructing patients on self-care after an insertion.
3. How do nurses know if a chest tube device has an air leak?
Answer: If the water seal room continues to bubble, there is an air leak. Nurses should inspect all tubing connections and the catheter insertion site to identify the leak. If the leak doesn’t go away, they should call the healthcare provider.
4. How does a chest-draining system tidal flow, and why is it important?
The patient’s breaths cause the water level in the water seal room to rise and fall. We call this phenomenon “tideling.” In this case, it means that the method is legal and working. The absence of tidaling may indicate a blockage or the lung’s full reopening.
5. If a chest tube comes loose by chance, what should a nurse do?
Answer: Put a clean petroleum gauze covering over the insertion site right away, watch the patient to make sure they aren’t having trouble breathing, and call the doctor or nurse. Do not try to put the tube back in without a doctor’s permission.
6. When and how should the nurse remove the chest tube?
Answer: The chest tube is taken out when it is proven that the lungs have re-expanded, there is little drainage, and there is no air leak. Nurses assist by preparing the patient, alleviating pain, ensuring proper positioning, and applying an occlusive covering following the removal of the dressing.
7. What information should the nurse record about chest tube drainage?
Answer: Write down the date, time, tube size, condition of the site, suction settings, type and amount of drainage, air leaks, patient reaction, and respiratory status. Charting correctly makes sure that care is safe and uniform.
8. What should nurses look out for as signs of problems with a chest tube?
Observe for sudden shortness of breath, increased pain, subcutaneous emphysema, signs of infection at the site of insertion, and excessive drainage (>100 mL/hour). These could all be signs of a major problem.
9. What steps should nurses take to keep chest tubes from causing infections?
Answer: Change the dressing in a clean way, wash your hands, keep the drainage system closed and below chest level, check the site every day, and don’t touch the tube more than necessary.
10. Can a nurse clamp a chest tube? If so, when should they do it?
Answer: You should only clamp when your doctor tells you to or when you need to locate the source of an air leak. Routine tightening can cause a tension pneumothorax, so only perform it when it is clearly necessary.